Fill in Your Cna Shower Sheets Form
PDF Forms Hub
Fill in Your Cna Shower Sheets Form
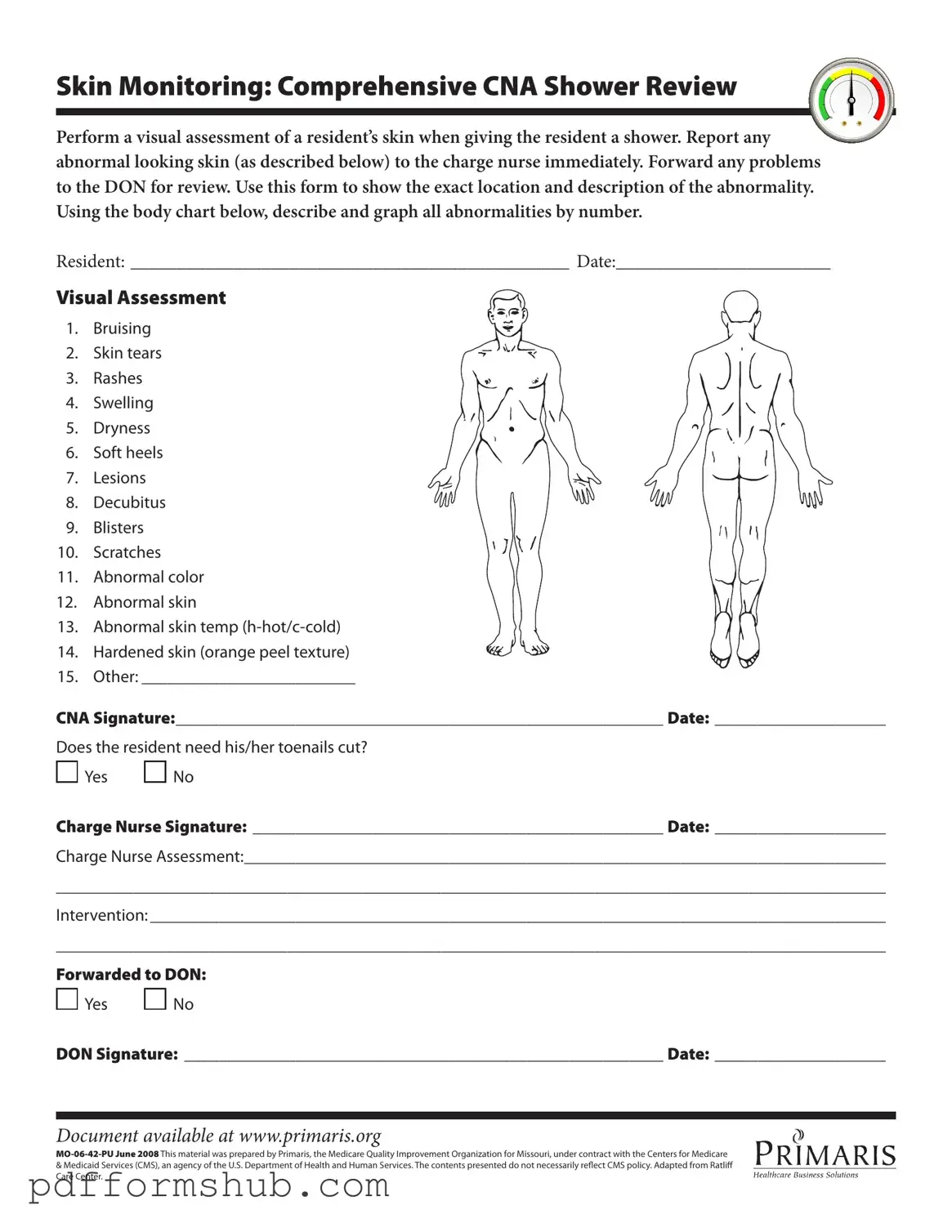
The CNA Shower Sheets form is a vital tool in ensuring the health and safety of residents during bathing activities. This form is designed to facilitate a thorough visual assessment of a resident's skin while they receive a shower. It emphasizes the importance of identifying and documenting any abnormalities, such as bruising, skin tears, rashes, and other skin conditions that may require immediate attention. By utilizing a body chart included in the form, certified nursing assistants (CNAs) can accurately pinpoint and describe these issues, allowing for effective communication with the charge nurse and the Director of Nursing (DON). This process not only ensures that any concerns are promptly addressed but also promotes a culture of proactive care. Additionally, the form includes a section for assessing the need for toenail care, further contributing to the overall well-being of the resident. Each signature on the form—from the CNA to the charge nurse and DON—serves to create a comprehensive record of the resident's condition and the interventions taken, reinforcing accountability and quality care within the facility.
The CNA Shower Sheets form is an essential tool for documenting the skin condition of residents during showers. However, several other forms and documents are often used in conjunction with it to ensure comprehensive care and accurate reporting. Below is a list of these documents, each serving a specific purpose in the care process.
Utilizing these forms alongside the CNA Shower Sheets enhances the quality of care provided to residents. Each document plays a critical role in maintaining accurate records, facilitating communication among staff, and ultimately ensuring the safety and well-being of those in care.
When filling out the CNA Shower Sheets form, attention to detail is crucial. Here are ten things to consider:
By adhering to these guidelines, you contribute significantly to the well-being of the residents and the overall quality of care provided.
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to assist Certified Nursing Assistants (CNAs) in conducting a thorough visual assessment of a resident’s skin during showering. This form helps document any abnormalities such as bruising, rashes, or skin tears, ensuring that these issues are reported to the charge nurse promptly for further evaluation.
What types of skin abnormalities should be reported?
CNAs should look for a variety of skin abnormalities, including:
How should CNAs document skin abnormalities?
CNAs should use the body chart provided on the form to graphically indicate the exact location of any skin abnormalities. Each abnormality should be numbered and described clearly to ensure that the charge nurse and Director of Nursing (DON) can understand the findings easily.
What should a CNA do if they find an abnormality?
Upon discovering any abnormal skin condition, the CNA must report it to the charge nurse immediately. It is essential to document the findings on the CNA Shower Sheets form and ensure that the charge nurse reviews the information for further action.
Is there a section for toenail care on the form?
Yes, the form includes a question regarding whether the resident needs their toenails cut. This is an important aspect of personal care, and the CNA should assess the condition of the resident's toenails during the shower.
What happens after the charge nurse reviews the form?
After the charge nurse reviews the CNA Shower Sheets form, they will provide their assessment and document any necessary interventions. If further action is required, the charge nurse may forward the information to the DON for additional review and follow-up.
Who is responsible for signing the form?
The form requires signatures from both the CNA who conducted the assessment and the charge nurse who reviewed it. Additionally, if the issue is forwarded to the DON, their signature is also required to confirm receipt and acknowledgment.
How can I access this document?
The CNA Shower Sheets form is available online at www.primaris.org. This ensures that CNAs can easily access the document for use in their daily routines.
What is the significance of the document's date?
The date on the form is crucial as it indicates when the assessment was conducted. This helps maintain accurate records and ensures that any follow-up actions are timely and appropriate.
Free Printable Dl-43 Form - Completion of the DL-43 is necessary for obtaining a state ID card.
In addition to its primary function, an Employment Verification Form can be enhanced with various resources to ensure completeness and accuracy. Employers can benefit from utilizing various templates that simplify the verification process, and useful resources like Templates and Guide can further assist in crafting effective forms for their needs.
Death of Joint Tenant California - This document may need to be recorded with the county recorder's office to be effective.
| Fact Name | Details |
|---|---|
| Purpose of Form | This form is used by Certified Nursing Assistants (CNAs) to document the visual assessment of a resident's skin during showering. |
| Skin Monitoring | CNAs must perform a thorough visual assessment of the resident's skin and report any abnormalities immediately to the charge nurse. |
| Abnormalities to Report | Common skin issues that need to be documented include bruising, skin tears, rashes, swelling, dryness, soft heels, lesions, decubitus ulcers, blisters, scratches, abnormal color, and temperature. |
| Body Chart | The form includes a body chart where CNAs can graphically indicate the location of any identified abnormalities by number. |
| Toenail Care | The form includes a section to indicate whether the resident needs toenail care, with options for 'Yes' or 'No.' |
| Charge Nurse's Role | The charge nurse must review the CNA's assessment and sign the form, providing their assessment and any necessary interventions. |
| Forwarding to DON | Any identified problems must be forwarded to the Director of Nursing (DON) for further review and action. |
| Documentation | This form serves as an important record of the resident's skin condition and care, which is vital for ongoing health assessments. |
| Governing Laws | This form is governed by regulations related to nursing home care and resident health standards, which vary by state. |